
House passed HR 4's negotiate prices for Medicare Drugs Bill -- but it is flawed (William Chirolas)
Categories

William Chirolas -- World News Trust
Jan. 15, 2007 -- Well, the House has passed HR 4, the Medicare drug reform that that will require Health and Human Services Secretary Michael Leavitt to negotiate prices on behalf of 29.4 million Medicare recipients, but leaves out the structure that allows that negotiation to result in lower prices -- the structure the Veteran's Administration uses for drug purchases, an approach that has been so successful in getting a lower price for drugs in that system.
Tony Snow is quoted last week as saying that the actuaries (and I am an actuary) at both the budget office and the Department of Health and Human Services say the bill will have little or no effect on federal spending and provide no substantial savings to the government.
And indeed CBO estimates that H.R. 4 would have a negligible effect on federal spending because they assume the Secretary would be unable to negotiate prices across the broad range of covered Part D drugs that are more favorable than those obtained by PDPs under current law, because the legislation specifically directs the Secretary to negotiate only about the prices that could be charged to PDPs, and explicitly indicates that the Secretary would not have authority to negotiate about some other factors that may influence the prescription drug market, we assume that the negotiations would be limited solely to a discussion about the prices to be charged to PDPs.
Given that the Secretary is not allowed to establish a formulary, there is little ability to encourage the use of particular drugs by Part D beneficiaries, so there is little leverage to obtain significant discounts.
It is not the Federal Government in his negotiations with drug manufacturers that will determine prices -- it will remain the negotiations between drug manufacturers and PDPs. Indeed PDPs are allowed to establish formularies -- subject to certain limits -- and thus have some ability to direct demand to drugs produced by one manufacturer rather than another. Paul Spitalnic, while not a fully credentialed actuary (he is an Associate of the Society of Actuaries and has a few exams to go before he would be called a fully accredited "Fellow of the Society of Actuaries) is not known to me to be incompetent, and if as decent as the likewise limited credentialed Chief Actuary of the Social Security System, I would have no problem trusting. Paul is the Director of the Parts C and D Actuarial Group in the Office of the Actuary at the Centers for Medicare and Medicaid Services, and he also says "the inability to drive market share via the establishment of a formulary or development of a preferred tier significantly undermines the effectiveness of this negotiation. Manufacturers would have little to gain by offering rebates that aren't linked to a preferred position of their products, and we assume that they will be unwilling to do so." ( Email:
So that is why there is no cost savings shown for this bill in the CBO and the Dept of Health and Human Services analysis -- granted these areas are administration control, not non-partisan areas, and might be considered bias in their analysis -- but Paul's comments are controlled by the Professional guidelines of the Society of Actuaries and should be trusted.
An analysis by the Washington Post of a report that Medicare pays 58 percent more for the most commonly prescribed medications than does the Department of Veterans Affairs, which negotiates directly with pharmaceutical companies, says the comparison is not apples-to-apples for several reasons, but a big difference is the limited choice in the VA program -- the same reason that is cited by Paul as his reason for not seeing a cost savings.
Why did HR 4 not follow the Veteran's Administration procedure that is copied in the Stabenow-Kennedy bill (which established a standard, limited as to choice, prescription drug benefit administered directly by Medicare, with seniors who choose this option getting only a modest deductible and co-payments for prescriptions, without any gaps in coverage, along with protection against drug costs above $5,100 per year)? So who wrote the "Medicare Prescription Drug Price Negotiation Act of 2007" that sounds so good in requiring Health and Human Services Secretary Michael Leavitt to negotiate prices on behalf of 29.4 million Medicare recipients who are covered through private stand-alone plans and Medicare managed-care plans - but then forbids a formulary? Are the House Democrats that stupid, or just afraid of offering a limited "choice" in a low cost package?
Perhaps the drug companies got to the Democrats? The U.S. drug companies spent $60 billion on research and development last year, and a low cost purchase, albeit limited to certain drugs, approach, has been estimated by the conservative Manhattan Institute as likely cutting $200 billion from drug-industry research budgets over the next 18 years. Of course, any such revenue cuts could easily be made up by cuts in marketing and advertising or by focusing research on innovative therapies rather than so-called "me too" drugs, which are slightly modified versions of existing medications. With those savings there would be no need to cut research budgets. But perhaps some Democrats really are afraid of the Drug company warnings of lost development of new drugs if Medicare does not pay the highest possible price?
The Senate can fix all the problems, but HR 4 is a disappointing effort by the House to get a better and cheaper medicare drug benefit.
***
House approves Medicare negotiations with drug manufacturers
The Associated Press Friday, January 12, 2007
Despite President Bush's veto threat, the House approved legislation Friday that would require the government to negotiate with drug companies over the price of medicines for Medicare participants.<snip>
But Republicans counter that there wouldn't be any savings. Also, the nonpartisan Congressional Budget Office said the legislation was unlikely to result in savings to taxpayers.
The drug program cost about $30 billion in its first year. Insurance companies offer competing coverage plans, and seniors may enroll in the one they like best. The administration announced on Wednesday that 23.5 million seniors had enrolled in stand-alone plans as of Jan. 1.
White House press secretary Tony Snow noted that actuaries at both the budget office and the Department of Health and Human Services say the bill will have little or no effect on federal spending and provide no substantial savings to the government.<snip>
-
CreatedMonday, January 15, 2007
-
Last modifiedWednesday, November 06, 2013
World Desk Activities

www.niemanlab.org/2024/04/inside-newsweek-ai-exper…

www.journalismfestival.com/programme/2024/reader-r…

Reader revenue beyond the English language – – International Journalism Festival
In the past few months, many news publishers in the US have announced layoffs. Others have tweaked or abandoned their paywalls and pursued more open models.…
phys.org/news/2024-04-surf-clams-coast-virginia-re…

Surf clams off the coast of Virginia reappear and rebound
The Atlantic surf clam, an economically valuable species that is the main ingredient in clam chowder and fried clam strips, has returned to Virginia waters…
medicalxpress.com/news/2024-04-antibiotics-reveal-…
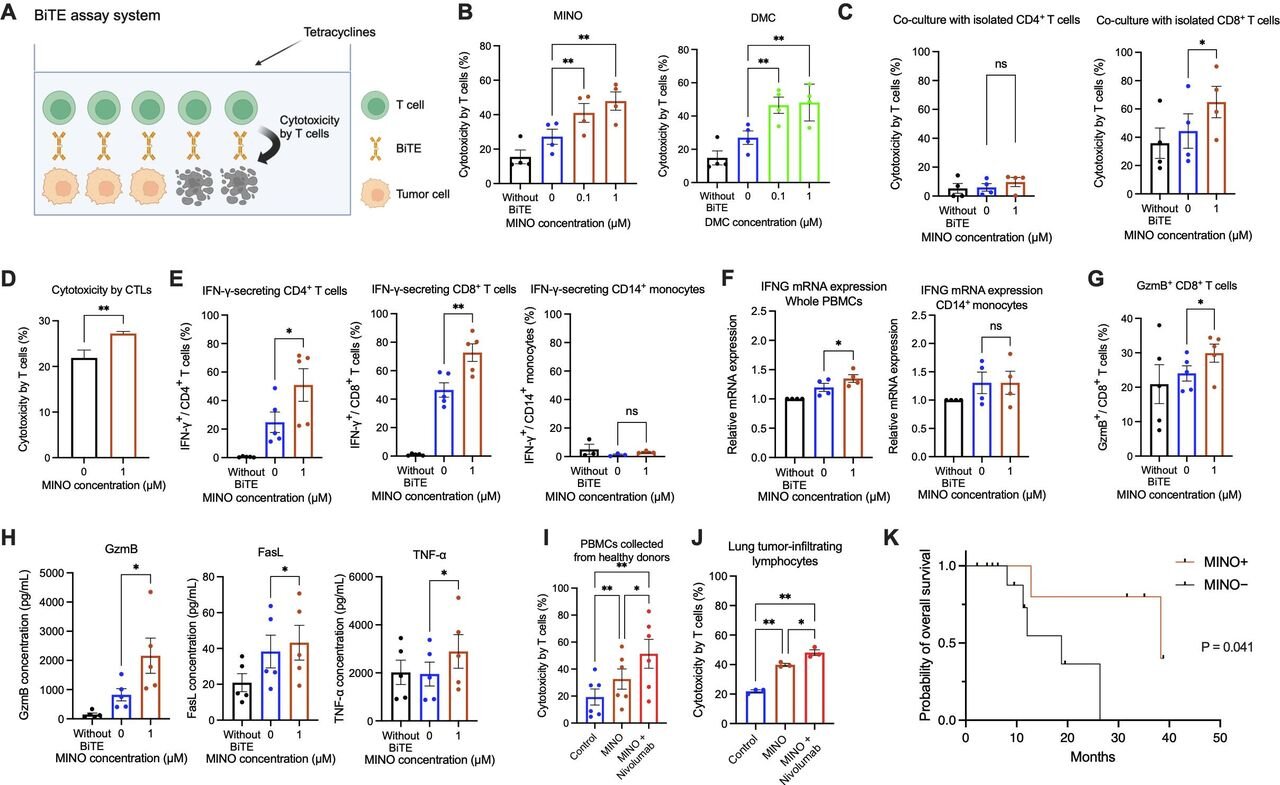
Antibiotics reveal a new way to fight cancer
Cancer cells grow and spread by hiding from the body's immune system. Immunotherapy allows the immune system to find and attack hidden cancer cells, helping…
phys.org/news/2024-04-crucial-quantum-internet.htm…
Crucial connection for 'quantum internet' made for the first time
Researchers have produced, stored, and retrieved quantum information for the first time, a critical step in quantum networking.
medicalxpress.com/news/2024-04-women-major-complic…

Women who experience major complications during pregnancy found to have increased risk of early death years later
A team of medical researchers from the University of Texas Health Science Center, in the U.S., and Lund University, in Sweden, has found via study…
medicalxpress.com/news/2024-04-common-hiv-treatmen…
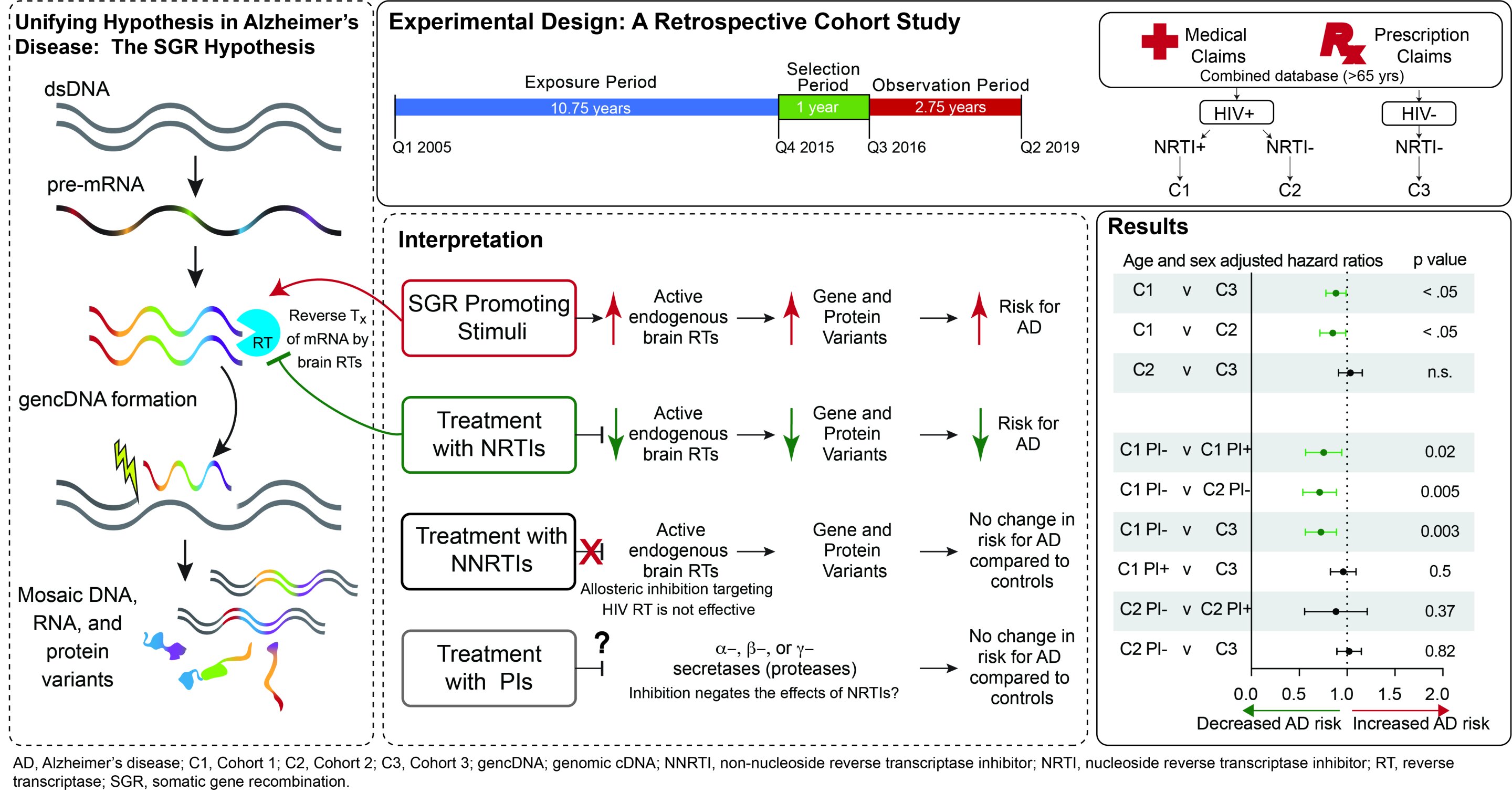
Common HIV treatments may aid Alzheimer's disease patients
Alzheimer's disease (AD) currently afflicts nearly seven million people in the U.S. With this number expected to grow to nearly 13 million by 2050, the…
medicalxpress.com/news/2024-04-adolescent-stress-p…

Study suggests adolescent stress may raise risk of postpartum depression in adults
In a new study, a Johns Hopkins Medicine-led research team reports that social stress during adolescence in female mice later results in prolonged elevation of…
medicalxpress.com/news/2024-04-positive-effect-mel…
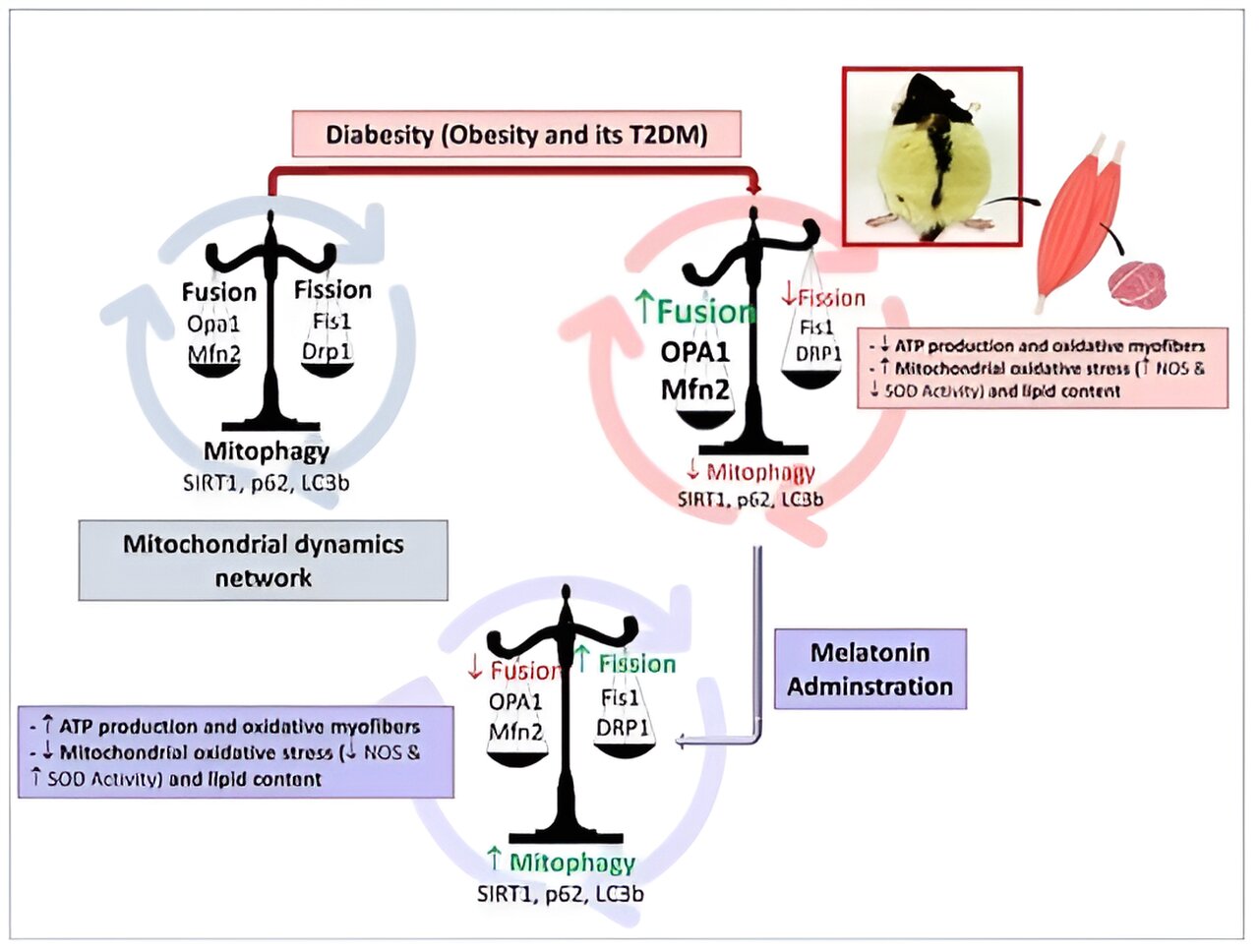
Researchers demonstrate the positive effect of melatonin in the prevention of obesity
Two international studies led by the University of Granada (UGR) have confirmed that melatonin helps prevent obesity. In addition, its effects are positive against visceral…
medicalxpress.com/news/2024-04-fecal-transplants-p…
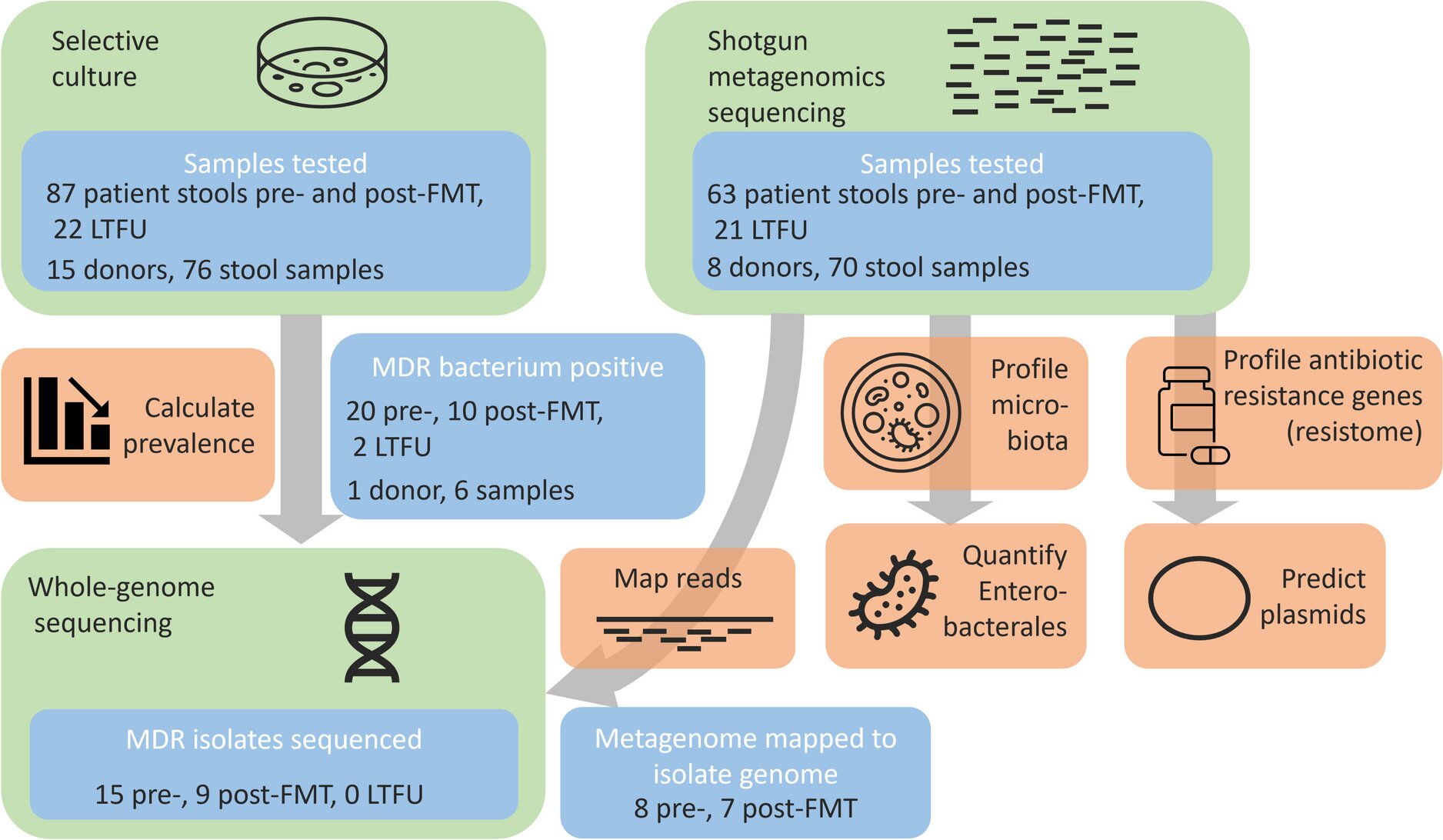
Researchers conclude fecal transplants can rid patients of resistant gut bacteria
Transferring fecal microbiota from healthy donors to the intestines of chronically ill people has beneficial effects on these recipients' gut bacteria, also in the longer…
Latest Stories







Electronic Frontier Foundation
-
Two Years Post-Roe: A Better Understanding of Digital Threats
April 18, 2024
-
Fourth Amendment is Not For Sale Act Passed the House, Now it Should Pass the Senate
April 18, 2024
-
About Face (Recognition) | EFFector 36.5
April 17, 2024
-
How Political Campaigns Use Your Data to Target You
April 16, 2024
The Intercept
-
U.S. Troops in Niger Say They’re “Stranded” and Can’t Get Mail, Medicine
April 18, 2024
-
Columbia Suspends Ilhan Omar’s Daughter One Day After Omar Grilled School Administrators
April 18, 2024
-
The Secret U.S. Alliance That Defended Israel From Iran Attack
April 18, 2024
-
The Gaping Hole in Supreme Court Rules for Tracking Links Between Litigants and Influence Groups
April 18, 2024
VTDigger
-
David Blittersdorf: H.289 has good intentions, but one big flaw
April 19, 2024
-
After a flood and a pandemic, Montpelier businesses continue to struggle
April 18, 2024
-
James Parker granted parole for his role in Dartmouth professors’ stabbing deaths
April 18, 2024
-
Final Countdown: All gifts matched up to $500
April 18, 2024
Mountain Times -- Central Vermont
-
The Mountain Times – Volume 51, Number 16 – April 17-23, 2024
April 17, 2024
-
Weekly Horoscope: April 17-23, 2024
April 17, 2024
-
Bookstock cancels summer event after 14 years
April 17, 2024
-
Crêpe breakfast tradition at sport hill
April 17, 2024
